
A bombshell study in America — from the National Institutes of Health and Moderna, no less — shows that unvaccinated people are much more likely to develop broad antibody immunity after Covid infections than people who have received mRNA shots. The gap remains large whether people had mild, moderate, or severe Covid infections, the study showed — undercutting a crucial argument that vaccine advocates have made to defend the shots.
BY Alex Berenson and Dr. Robert Malone for The International Chronicles
The research draws on data from Moderna’s 30,000-person clinical trial for its mRNA shots. It may help explain why so many Americans now suffer multiple Covid infections, sometimes within months.
Researchers already knew that many vaccinated people do not gain antibodies to the entire coronavirus after they are infected with Covid.
Unvaccinated people nearly always gain antibodies to the nucleocapsid protein, which covers the virus’s core of RNA, as well as its spike protein, which allows the virus to attack our cells. Vaccinated people often lack those anti-nucleocapsid antibodies and only have spike protein antibodies.
Vaccine advocates claim the lack of nucleocapsid antibodies may occur because the mRNA shots prime people to fight off the Covid infections more quickly and have lower viral loads. In this view, the narrow immune response is a feature, not a bug – vaccinated people are less seriously infected and so do not need to generate anti-nucleocapsid antibodies.
This study essentially demolishes that theory.
Scientists from the National Institutes of Health and Moderna quietly posted the paper in April of 2022 as a pre-print, but it has received little attention despite its import.
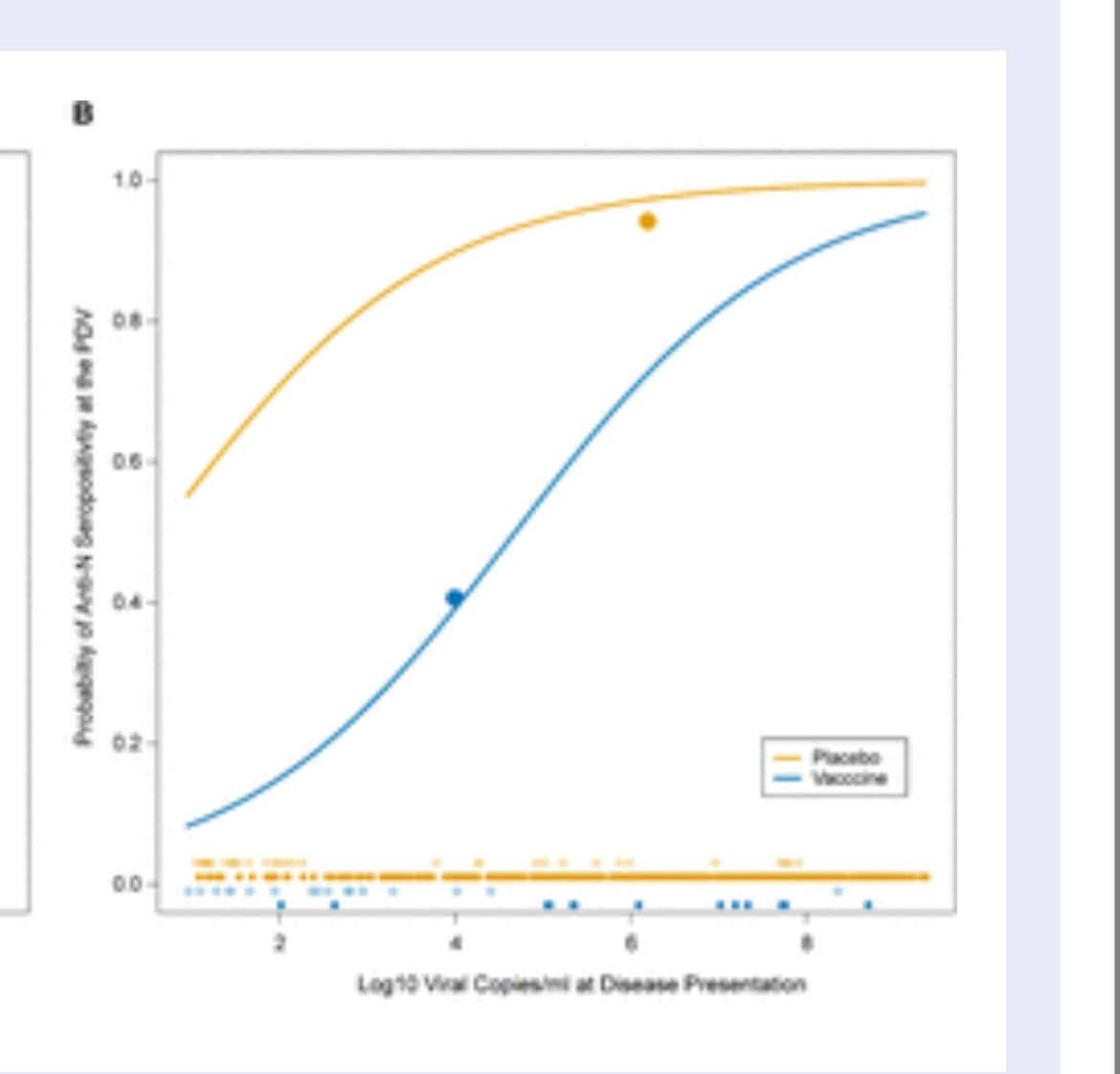
The researchers examined the development of anti-nucleocapsid antibodies in people who had been part of Moderna’s clinical trial and were infected with Covid. As they expected, the scientists found that the vaccinated people were far less likely to develop the anti-nucleocapsid antibodies. Only 40 percent of people who received the shots had antibodies, compared to 93 percent of those who did not.
But they then went a step further. Because the infected people had been in the trial, their viral loads had been precisely measured when they were found to have Covid. So the researchers were able to compare vaccinated and unvaccinated people who had the same amounts of virus in their blood.
Once again, they found that unvaccinated people were far more likely to develop anti-nucleocapsid antibodies than the jabbed. An unvaccinated person with a mild infection had a 71 percent chance of mounting an immune response that included those antibodies. A vaccinated person had about a 15 percent chance.
Only in cases of severe infection and very high viral loads did the difference narrow significantly; in those cases all unvaccinated people and most of the vaccinated had anti-nucleocapsid antibodies.
The chart that should worry the vaccinated: the yellow line shows the odds that an unvaccinated person will develop anti-nucleocapsid antibodies to Sars-Cov-2, stratified by viral load. The blue line shows the same odds for a person who received an mRNA shot.
An unvaccinated person has an almost 60 percent chance of developing antibodies even with an extremely mild infection; a vaccinated person needs almost 100,000 times as much virus in his blood to have the same chance.
The researchers also tried to correlate the development of anti-nucleocapsid antibodies with viral load over time. Theoretically, if vaccinated people cleared the virus more quickly, they might have fewer antibodies – another version of the “it’s-a-feature-not-a-bug” defense. But they found the opposite – again, vaccination status and not the duration of infection was what mattered.
The “likely explanation is a vaccine-induced reduction in seroconversion [the production of antibodies],” the researchers wrote.
The study all-but-proves the mRNA shots themselves — and not whatever reduction in viral loads they may cause — are impeding the development of the anti-nucleocapsid antibodies.
Still, the long-term immunological and medical significance of the lack of those antibodies is less clear. The reason that drugmakers targeted the spike protein rather than the nucleocapsid in the first place is that Sars-Cov-2 depends on its spike for its crucial initial attack on the exterior of human cells. It exposes the nucleocapsid protein only after it has dumped its mRNA inside the cell itself.
Yet there is some evidence that antibodies to the nucleocapsid play an important role later in our immune response.
And the coronavirus’s spike protein mutates rapidly, potentially rendering antibodies it against useless. For example, Omicron’s spike is markedly different than that of earlier variants. The nucleocapsid protein mutates far more slowly, offering a potential second line of defense.
Answering these questions and figuring out what if any harm the lack of anti-nucleocapsid antibodies may cause will require a concerted research effort. But it is precisely this kind of work – work that might reveal long-term damage from the vaccines – that government and academic scientists are studiously avoiding.
In the meantime, expect lots more stories like this:

And expect those articles to avoid the most important question of all – whether unvaccinated people are being reinfected, or only the vaccinated.
SARS-CoV2 Spike protein is a toxin… factcheckers were wrong. People continue to suffer the consequences.
First, a quick overview of the various “factchecking” organization statements. How many people developed brain damages or lost their life or that of a loved one because of accepting a vaccine based on the falsehoods propagated by these grossly unqualified “factcheckers”? Do they have criminal liability for their falsehoods and propaganda?
As you look through this, please keep in mind that the FDA has approved three doses of these mRNA vaccines for administration to all of our 5-11 year old children. Under emergency use authorization, of course. Even though there is no medical emergency.
Factcheck.org
COVID-19 Vaccine-Generated Spike Protein is Safe, Contrary to Viral Claims
Posted on July 1, 2021. Link here.
Catalina Jarmillo’s training is from the Columbia School of Journalism.
Why would anyone place any credence in what she has to say about toxicology and molecular virology? How many excess deaths can be attributed to this lie?

Politifact
No sign that the COVID-19 vaccines’ spike protein is toxic or ‘cytotoxic’
POLITIFACT CONTRIBUTING WRITER
Tom Kertscher is a contributing writer for PolitiFact. Previously, he was a fact-checker for PolitiFact Wisconsin.
You can find this article here.
And why would anyone believe Tom Kertscher, who has no training in medicine or biology, let alone molecular virology? And why is a political fact checking site making assessments about biology and toxicology anyhow?

Associated Press
Spike protein produced by vaccine not toxic
By BEATRICE DUPUY
June 9, 2021
Another doozey. You can find it here.

Now, let us review the actual science.
Not what these wannabe scientists who are actually journalists at best claim to be true.
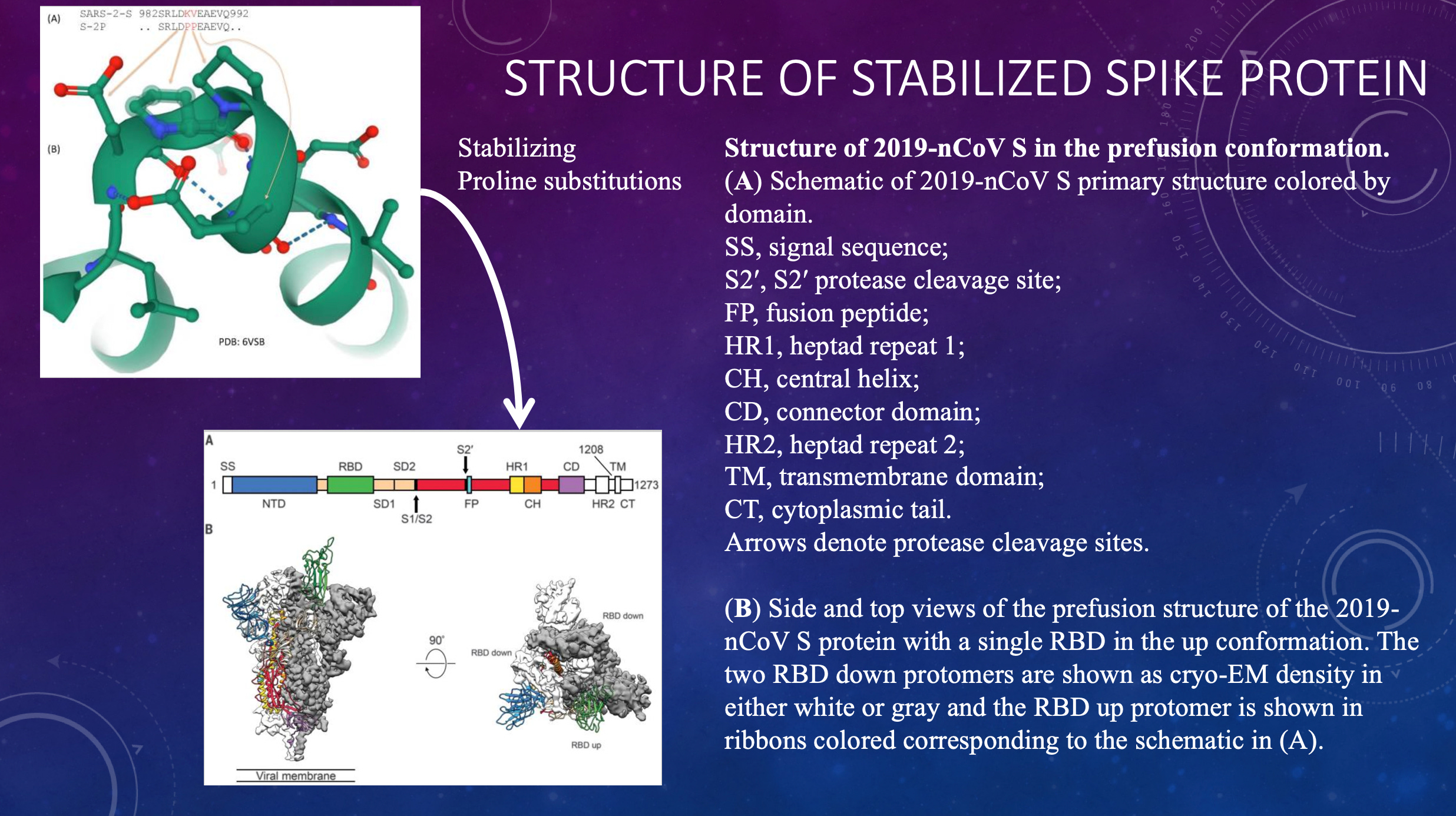
First off, it is important to understand a little bit about the SARS-CoV-2 Spike protein.
The only difference in the actual protein sequence between the original “Wuhan” strain Spike protein of the virus, and that coded for by the genetic vaccines, is two amino acids which have been changed in the S2 region of the protein. These were not introduced to make that vaccine version less toxic (as some “factcheckers” have asserted), but rather to make it better able to stimulate an antibody-based immune response. Whether vaccine encoded or virus encoded, the S1 subunit (which includes the receptor binding domain (to which the majority of “neutralizing” antibodies are directed) gets cut free (“proteolytically cleaved’) to yield an S1 subunit which is free to circulate in the blood, bind ACE2 receptors, interact with platelets, neurons, open up vascular endothelial tight junctions etc. THERE IS NO DIFFERENCE BETWEEN THE S1 SUBUNIT RELEASED FROM THE VACCINE SPIKE PROTEIN AND THE S1 SUBUNIT RELEASED FROM THE VIRUS SPIKE PROTEIN. THEY ARE THE SAME DAMN THING!
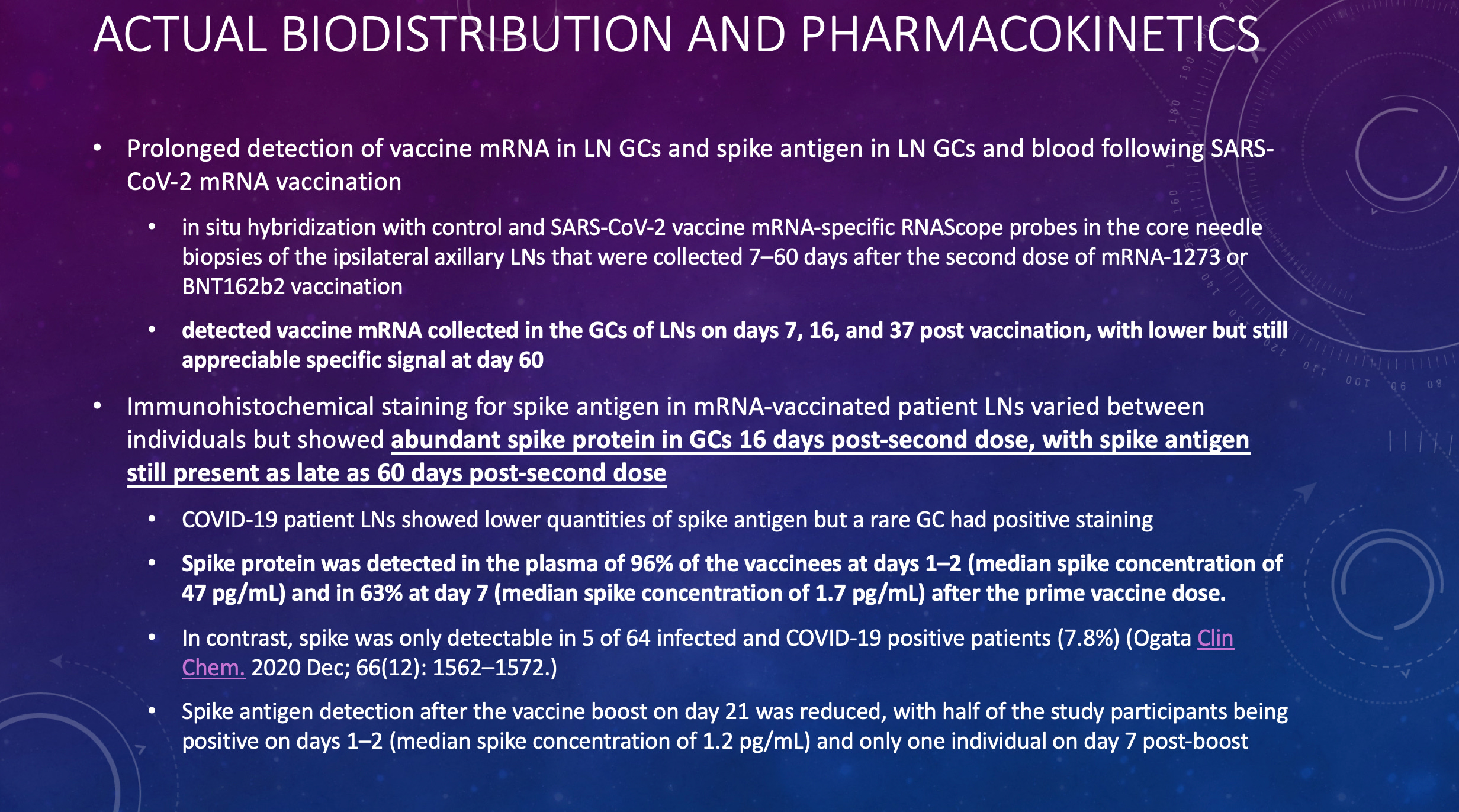
Now, how much and for how long does this free S1 subunit spike protein, including the receptor binding domain, become produced by the mRNA vaccines, versus how much and for how long by natural infection?
Surely this was well understood and characterized by Pfizer before these vaccines were widely deployed? Surely the FDA required that these studies be performed?
NOPE. WE HAD TO WAIT UNTIL AN ACADEMIC GROUP DID THE STUDIES AND PUBLISHED AT THE END OF JANUARY 2022. AND BURIED THE FINDINGS BY USING AN OBSCURE TITLE.
WELL, ISN’T THAT INTERESTING.
So, the vaccine produces far more spike S1 subunit for far longer than the natural infection does. Hmm. Curiouser and curiouser.
But is the S1 subunit (which is identical between the virus and the vaccine) actually a toxin? Good question. Let’s look into that. One moment…. searching. There.
First question – does spike S1 subunit get into the brain across the blood brain barrier?
Why yes, Virginia, thank you for asking. It does! You are such a good student.
You can find and read the article yourself here.
Next question. Does Spike S1 do any damage to the brain when it hits nerve cells (neurons)? Oops. Looks like it does! Who would have guessed. Well, who among those scientists who are not misinformation spreaders?
Read it for yourself here.
AND THEN THERE IS THIS ONE.
Read this one here.
Highlights
•COVID-19 generates cerebrovascular, sensitive, motor, cognitive and diffuse brain disorders.
•The trigeminal and vagus nerve or the gut-brain axis are the entrance of SARS-CoV-2 in brain.
•SARS-CoV-2 affects brain by neuroinvasion and by the consequences of the systemic infection.
•COVID-19 favors BBB disruption, inflammation, hypoxia, and secondary infections.
•The study of the neurological affectation of COVID-19 raises a new challenge for neuroscience.
For this one, it is important to recognize that there is no significant difference between the symptoms of long COVID (PASC) and post vaccination syndrome.

And you can read all about it here.
And then there is this little issue of demyelination of nerve cells. That is sort of like stripping off the insulation on a wire. Causes short circuits and all sorts of problems.
Yipes. Read here.
And brain endothelial attack. What could possibly go wrong?
Which you can read here.
SO, I ASK YOU, WHO WAS RIGHT? THE SCIENTISTS OR THE FACTCHECKERS?
IS THE SPIKE S1 SUBUNIT PRESENT IN BOTH VIRUS AND THE PRODUCT OF THE GENETIC INOCULATIONS A TOXIN?
“A toxin is a harmful substance produced within living cells or organisms;[1][2] synthetic toxicants created by artificial processes are thus excluded.[3] The term was first used by organic chemist Ludwig Brieger (1849–1919)[4] and is derived from the word toxic.”